A whole body FDG PET scan was also performed to look for any distant metastases, which was negative
Discussion
History
Henry K. Pancoast in 1924 first described this clinical entity of “apical chest tumors”. Pancoast tumours are neoplasms of pulmonary origin located at the apical pleuropulmonary groove (superior sulcus). Superior sulcus tumour term is now not used. They account for about 3 – 5% of all bronchogenic carcinomas.
More than 95% of Pancoast tumors are usually non-small cell carcinomas. Previously squamous cell carcinoma was considered predominant histological type, however recent studies show adenocarcinoma as most common type. Small cell carcinomas are seen in fewer than 5% of cases.
The unique feature of Pancoast tumors appears not to lie in the tumor biology, but rather in the anatomy of the region.
Clinical Features :
The usual symptoms of lung cancer like cough, dyspnea and hemoptysis are usually absent due to the peripheral location of tumor in the lung apex. Classically these tumors present with pancoast syndrome, however is seen in only about one third of the patients. Pancoast syndrome is characterized by ipsilateral shoulder and arm pain, paresthesias, paresis and atrophy of the thenar muscles of the hand, and Horner syndrome (ptosis, miosis, and anhidrosis) and occurs due to involvement of the inferior portion of the brachial plexus. Pancoast tumors can also involve intercostal nerves, stellate ganglion, adjacent ribs and vertebrae.
A cervical radiculopathy or a cuff-rotator lesion is a common clinical bias.
Superior vena cava syndrome or recurrent nerve palsy may occur as late complications of the disease progression.
Role of Imaging :
Because of the wide range of clinical presentations, the role of imaging is pivotal in the diagnosis and evaluation of the therapeutic approach.
Imaging findings include lung apical mass with or without bone destruction, mediastinal extension, extra-thoracic extension to involve brachial plexus and stellate ganglion.
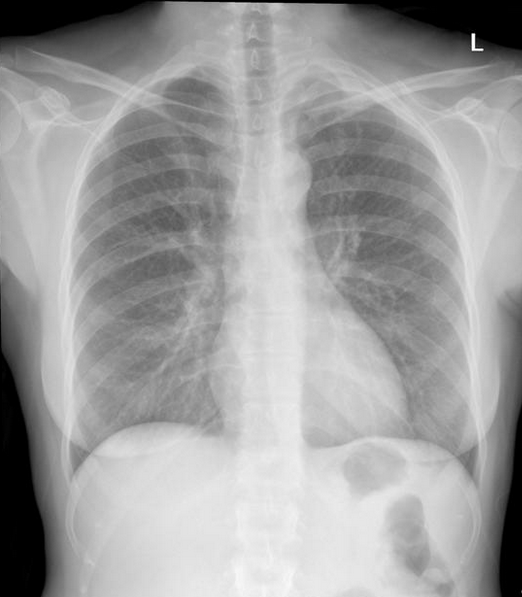
Chest radiography – The ordinary chest films or apical lordotic views may depict apical mass , but often do not show the bone destruction, however , can many times be easily recognized by the addition of an AP view of the lower cervical-upper dorsal spine. Lung apex is considered as a review area on all chest radiograph interpretations.
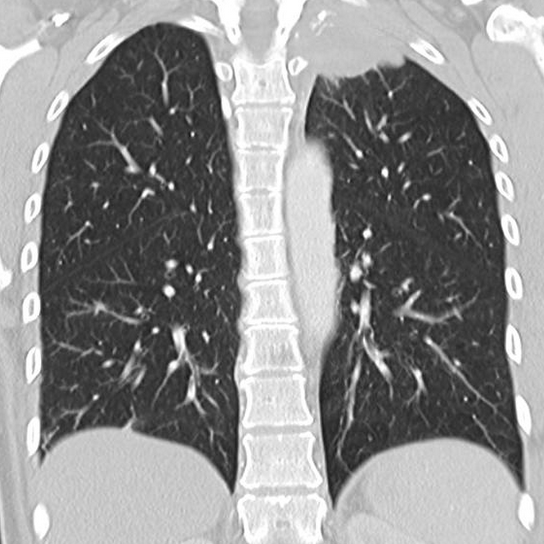
Computed tomography – CT is the gold standard imaging technique, especially for the evaluation of the bone erosion (vertebral body and rib involvement), evaluation of the intrathoracic structures (particularly the mediastinal adenopathy) and extra-thoracic extension.
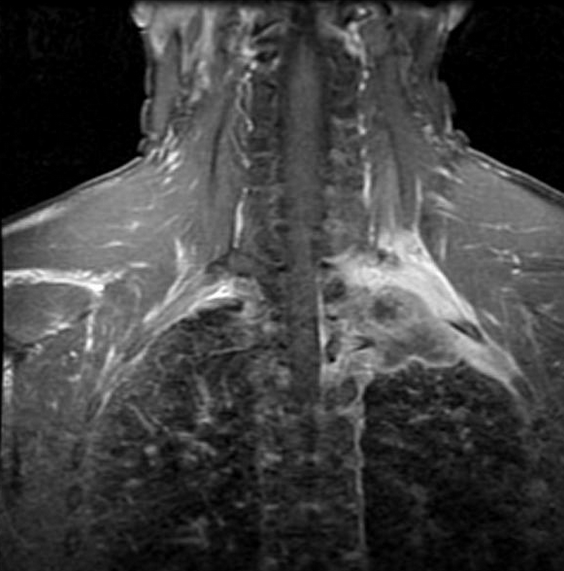
MRI – For evaluation of loco-regional extension (particularly brachial plexus, subclavian vessels, parietal pleura, subpleural fat, neuro vertebral foramina, and spinal canal)
Intravenous contrast medium ( in both CT & MRI) is helpful for the assessment of a vascular invasion . It may also help to distinguish between post treatment fibrosis and recurrence of the neoplasm.
PET-CT- Helps in assessing nodal and distant metastases. PET-CT also helps in accurate delineation of the gross tumor volume, which will be essential for the radiation treatment planning.
Therapeutic options:
Pancoast tumors were once considered universally fatal. However, improvements in multi modality therapy and the development of new techniques for resection have made curative treatment possible for these tumors.
Trimodality approach is now accepted as the new standard of care for the management of Pancoast tumors. Induction concurrent chemoradiotherapy followed by complete surgical resection aims to control the primary tumor, loco-regional lymphatic extension and to lower the stage of locally advanced tumors and have reported to improve the 5-year survival rates up to 44-56%.
Absolute contraindications for surgery are brachial plexus invasion at a level above the T1 Nerve, Vertebral body invasion > 50%, invasion of the esophagus or trachea, distant metastases, mediastinal or contralateral supraclavicular nodal metastases.
Article Info
Published on 01.10.2023
Corresponding Author: Dr Arun Mohan M, Dept of Radiology, SUT Hospital Pattom, Trivandrum, Kerala, India, email : arunmohandr@gmail.com, phone: 9400044433
How to cite this article: Arun Mohan M, Multi-modality Imaging features in Pancoast tumour. JAMST. 2023; 1(1): 23 – 25